




Airways
October – December 2018
MTSA faculty present research at European Society of Regional Anaesthesia Congress
Annual event focuses on breakthroughs in the field regional anesthesia and pain therapy
Above photo: MTSA alumni John Edwards (left) and Stace Dollar (right) traveled to the 37th Annual European Society of Regional Anaesthesia (ESRA) Congress held in Dublin, Ireland, to present their pain management research study. Also pictured is their colleague and one of the study’s co-authors, Dr. Thomas Young.
MTSA’s Acute Surgical Pain Management (ASPM) Fellowship Director and three ASPM Fellows submitted research studies that were accepted at the 37th Annual European Society of Regional Anaesthesia (ESRA) Congress held in Dublin, Ireland, in September – a first for the School.
The two separate studies conducted by Stace Dollar, MS, CRNA; John Edwards, MS, CRNA; Bill Johnson, DNAP, CRNA; and Kelly Martin, MS, CRNA, focused on new techniques and protocols that improve pain management for patients undergoing breast surgery.
Dollar and Edwards, both MTSA alumni, traveled to Dublin in connection with their research, Retrospective Comparison of Traditional and Enhanced Recovery After-Surgery Protocols Among Women Undergoing Mastectomy.
Johnson and Martin’s study, Retroclavicular Approach to the PECS (RAP) Block: A Novel Regional Technique for Breast Surgery, was also featured in the research package offered to ESRA Congress participants. Martin and Johnson also traveled to the event for the presentation.
All four presenters have ties to MTSA’s Acute Surgical Pain Management (ASPM) Fellowship; Johnson is director of the program, while Dollar, Edwards and Martin are part-time faculty.
“This is a major milestone for MTSA and the ASPM Fellowship,” Johnson said. “It shows that not only are we able to educate CRNAs, but we can help facilitate this type of cutting-edge research, which has enormous benefit to the anesthesia community around the world. There will be much more original research like this coming out of the Fellowship.”
According to Johnson, one of the key elements to advancing knowledge and producing quality research is MTSA’s cadaveric courses, in which CRNAs can try new techniques and increase their proficiency and efficacy.
“Our cadaveric courses give us a platform for Fellows to come back to Nashville and participate in some of these advanced techniques. The cadaveric models enable them to do the imaging, needling, distribution of local anesthetic, placement of catheters, and more. It’s about as high-fidelity as you can get in terms of educating and reproducing the results clinically,” Johnson said.
The ASPM Fellowship has provided a unique opportunity to grow professionally, according to Dollar. “John and I wouldn’t be where we are today had we not become involved with MTSA. It’s been a privilege to be part of the ASPM Fellowship. The Fellowship provides a big advantage for nurse anesthetists out in the field in rural areas, helping patients with their pain control and combatting the opioid crisis.”
Martin, who completed the Fellowship this year, was honored that his and Johnson’s study was accepted at the ESRA Congress and sees it as part of a larger effort: “The goal is to spark an interest in the anesthesia community that there’s a new pain management technique and see who might be able to start implementing it on patients, doing small case studies, and eventually taking it to larger trials. Many of the regional anesthesia providers that I admire and read were at the conference, so it was exciting to see their reaction and talk about the possibilities,” he said.
Edwards specifically chose the ESRA Congress to submit their abstract, due to its connection with several leading professionals in the field who are based in Europe. He said, “The block technique that we utilize in our project was actually developed by an anesthesiologist from Spain named Rafael Blanco, so I felt we learned that from him, he brought that to the forefront, and I wanted to present where many of these techniques have originated.”
According to Johnson, the Fellowship faculty members have plans to further develop their respective studies and submit them to multiple journals for review and potential publication, which will continue to grow the breadth and depth of scholarship being facilitated by MTSA.
“Having this research published and presented is an important step in advancing new approaches to acute pain management on a wide variety of patients. As we look at treatments and interventions for different types of surgeries, it will have a huge impact on patient care,” Johnson said.
Dollar and Edwards are CRNAs with Central Kentucky Anesthesia and practice at Baptist Health Lexington in Kentucky. Martin is a professor in the nurse anesthesia program at York College as well as full-time faculty member at Wellspan Health at York Hospital in Pennsylvania.
The annual ESRA Congress offers sessions and workshops led by world-renowned experts specializing in regional anesthesia and pain therapy. It aims to improve cooperative study to enable breakthroughs in the field.
More information on MTSA’s Acute Surgical Pain Management Fellowship and cadaveric workshops is available at www.mtsa.edu.

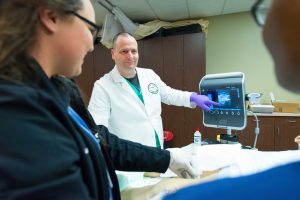
John Edwards provides instruction to attendees during a Cadaveric Ultrasound-Guided Regional Anesthesia Workshop at MTSA.

Bill Johnson (second from right) and Kelly Martin (right) demonstrate on a cadaveric specimen during an Ultrasound-Guided Regional Anesthesia Workshop at MTSA.

Bill Johnson, DNAP, CRNA, Director, Acute Surgical Pain Management Fellowship
About the Research Studies Presented at ESRA Congress
Following are details on the research studies conducted by four MTSA faculty members and submitted to the European Society of Regional Anaesthesia (ESRA) Congress held in Dublin, Ireland.
Retrospective Comparison of Traditional and Enhanced Recovery After Surgery Protocols Among Women Undergoing Mastectomy
Walid Abou-Jaoude, MD, Thomas J. Young, MD, John M. Edwards III, MS, CRNA, Stace D. Dollar, MS, CRNA, Heather Shearin, MS, CRNA, Barbara Self, BS, RN, OCN, Stacy Stanifer, APRN, MSN, AOCNS, Susan Germann Yackzan, APRN, MSN, AOCN
Background and aims:
Acute post-surgical pain is difficult to manage in patients undergoing breast cancer surgery. An ERAS protocol for mastectomy patients was developed in 2016. This study aims to compare pain scores, narcotic use, postoperative nausea and vomiting and antiemetic administration between postoperative mastectomy patients who received Traditional Recovery After Surgery (TRAS) or the ERAS protocol.
Methods:
A retrospective chart review of TRAS and ERAS for mastectomy surgery was designed. A statistical power analysis determined a necessary sample size of 102. Two groups were evaluated: 51 patients having mastectomy surgery from January to May 2016, prior to ERAS implementation, and 51 patients having mastectomy after implementation of ERAS protocols.
Results:
No significant differences were found between the groups in terms of demographics or pain history. A significant difference was found on POD0 between TRAS and ERAS groups in antiemetic use, mean and max pain scores with ERAS being significantly lower. Oral morphine equivalent intake was significantly less on POD0 and POD1 in the ERAS group. On POD0 the oral morphine equivalent was 58.3 mg for TRAS compared with 26.7 mg for ERAS and on POD1 was 20.8 mg for the TRAS group, significantly higher than the 4.7 mg average in the ERAS group.
Conclusions:
The incorporation of ERAS measures into the surgical care for mastectomy surgery can positively affect recovery. This ERAS protocol may improve pain control, reduce PONV, and reduce opioid adverse events.
Retroclavicular Approach to the PECS (RAP) Block: A Novel Regional Technique for Breast Surgery
Kelly Martin, MS, CRNA, and Bill Johnson, DNAP, CRNA
Background and aims:
Acute and chronic pain following breast surgery can be reduced when interfascial plane blocks of the chest wall are implemented as a part of perioperative analgesia. In this review, the literature was assessed evaluating the efficacy of the pectoral nerves (PECS) II block as an appropriate technique for breast analgesia. From this evidence-based review, a novel Retroclavicular Approach to the PECS (RAP) block is described which allows for preemptive catheter placement prior to surgical incision. Lastly, we present evidence of effective dye spread from an anatomical investigation in fresh cadavers utilizing the RAP technique.
Methods:
(a) Literature Review: Of the 805 articles screened for eligibility, 15 were included to determine the efficacy of the PECS II block for breast analgesia. (b) Cadaveric Dye Study RAP blocks were conducted on four human cadavers. Injections were made within the interfascial plane between the pectoralis muscles using 10 mL of dye in two cadavers, and within the interfascial plane between the pectoralis minor and serratus anterior muscles using 20 mL of dye in two cadavers. Catheters were placed in each of the four cadavers. Tissue dissection was then performed to determine the spread of injectate within anatomically relevant tissue specific to breast analgesia.
Results:
Compared to placebo, the PECS II block provides sufficient perioperative breast analgesia with less 24-hour opioid consumption and reduced pain scores for up to 48 hours postoperatively.
Conclusions:
In our cadaveric dye study, we reported satisfactory staining of nerves relevant to breast analgesia within respective interfascial planes using the RAP technique.
Research Study Discussions
Following are excerpts from conversations with the MTSA faculty who submitted research studies to the European Society of Regional Anaesthesia (ESRA) Congress held in Dublin, Ireland.
Retrospective Comparison of Traditional and Enhanced Recovery After Surgery Protocols Among Women Undergoing Mastectomy
Walid Abou-Jaoude, MD, Thomas J. Young, MD, John M. Edwards III, MS, CRNA, Stace D. Dollar, MS, CRNA, Heather Shearin, MS, CRNA, Barbara Self, BS, RN, OCN, Stacy Stanifer, APRN, MSN, AOCNS, Susan Germann Yackzan, APRN, MSN, AOCN

Edwards:
Enhanced Recovery After Surgery (ERAS) protocols, originally started in Europe, are now gaining momentum in the U.S. Those protocols look at how we take a patient through the perioperative period, which includes when you first find out you need surgery, perhaps a month ahead of time. Instead of just showing up for surgery, now we want the patient to focus on good nutrition and exercise in the weeks prior to surgery. When you show up for surgery, we want you to be hydrated with water or a sports drink with carbohydrates so your body isn’t completely in a starvation mode.
During surgery, we’ve traditionally used opioids to manage pain, including IV opioids in the OR and PACU (post-anesthesia care unit). Afterwards on the floor you might get more IV or oral opioids, which have many adverse effects including impaired cognitive function, constipation, nausea, vomiting and respiratory arrest. Now we want to manage pain from a multi-modal approach, which includes the use of acetaminophen and an NSAID in the preop room and providing regional anesthetic techniques, or nerve blocks, during surgery. The use of this multi-modal approach allows us to provide an opioid sparing anesthetic which leaves you feeling better after surgery. When you go to the floor to spend the night after surgery, we might make you walk into your room because we want you to ambulate as soon as possible. It’s good from a pain-management perspective to get active and moving. Then we keep you on a schedule of non-opioid medicine, such as acetaminophen every 6 hours, an NSAID twice a day, ice, elevating the body part, and ambulating up to 5 times a day. By doing all that, we can limit the amount of opioids you use, which then reduces all of the opioid-related adverse events. Then you’re able to do physical therapy. We advance your diet on the day of surgery to allow your body proper nutrition. You go home sooner. This is more of a wholistic approach. That’s the movement in ERAS.
In late 2015, Stace and I were part of a team led by one of our physician anesthesiologists, Dr. Thomas Broster, who developed the ERAS protocol at our facility for colorectal surgery. There was a lot of buzz in our hospital about that. So one of our general surgeons who does a lot of breast cancer surgeries approached us. He wanted these enhanced recovery programs for his breast cancer patients. So our ERAS development team spearheaded that project. We took what we learned in colorectal and applied it to breast cancer. We put the protocol together, launched it as a trial program in early 2016, and we saw really great results.
After that, Stace and I were asked to come to the monthly tumor board meeting and discuss this new protocol for breast cancer with people from hospital administration, surgeons, nursing staff, etc. Out of that meeting, they approached us and said they’d like to do a research project around this and look at the patients who received the traditional vs. enhanced recovery approach. We partnered with the surgeon, Dr. Walid Abou-Jaoude, and oncology research nurses Stacy Stanifer, APRN, MSN, AOCNS, and Susan Yackzan, APRN, MSN, AOCN. As a team we wrote an IRB application, and it was accepted. So we started that in 2016, and we’ve just now finished up all the data collection on it.
As far as our research results, we found a significant difference between ERAS and TRAS patients in four areas:
- Antiemetic use on POD0 (20% vs 41% p=0.018)
- Mean Pain Score on POD0 (1.9 vs 3.2 p ≤ 0.005)
- Oral Morphine Equivalent POD0 (26.7 vs 58.3 p ≤ 0.005)
- Oral Morphine Equivalent POD1 (4.7vs 20.8 p ≤ 0.005
So we really met our goals of reducing nausea and vomiting, reducing the amount of opioids, reducing pain scores and having a positive impact on patients’ lives.
The thought of implementing these ERAS techniques can be overwhelming. But I encourage people to “do for one what you wish you could do for everyone.” To me that means just implement it for the next patient you take care of. It may be as simple as ordering acetaminophen or ibuprofen in the preop room. Perhaps you don’t know how to do a PECs block, but you can learn by taking a course at MTSA. Do what you’d hope someone else would do for you or your family member undergoing surgery.

Dollar:
Our hospital has a really great research team, and they opened their doors to help us create this study. I recently found out that we only have one more case before all of our data is collected and we can complete the study. Hopefully in another six months it will be ready to be published.
In terms of how these new techniques will be received by the anesthesia community, I’m hopeful that a wide range of CRNAs will embrace them and start using them. It may be easier for those who’ve recently started practicing in the last few years because they are usually involved in newer techniques and research. CRNAs who have been practicing a long time may need a little more convincing. Often it’s a matter of “seeing is believing.” So as they see patients who have benefitted from these enhanced techniques, hopefully they’ll come onboard. That’s why I think it’s a good trend that more CRNAs are completing their doctorates and digging into the latest scholarship.
So much of what we’ve studied and implemented is tied to combatting the opioid epidemic. It’s something that we have to get control of. When a patient has excellent acute post-surgical pain management in the hospital utilizing a multi-modal approach, they may not need many opioid pain pills upon discharge. There’s a lot of data showing not every patient needs 50 Percocet pills when they are discharged; based on the procedure, they may only need 10 or 15. It’s a new approach that hopefully will steer providers away from the traditional choice of prescribing large amounts opioids that end up in our communities for misuse and diversion.
The bottom line is we must focus on providing excellent patient care. The challenge is making it possible to have every provider at every facility provide the same care. Not everyone has the resources or support that John and I have been lucky enough to have over the last five or six years.
Retroclavicular Approach to the PECS (RAP) Block: A Novel Regional Technique for Breast Surgery
Kelly Martin, MS, CRNA, and Bill Johnson, DNAP, CRNA

Martin:
This research began with an assignment for the Acute Surgical Pain Management Fellowship. I do a lot of breast procedures – mastectomies and reconstructions for patients with breast cancer. It’s fairly common for patients to have quite a bit of pain perioperatively, so we look for ways to help minimize the pain as much as possible. There are different regional anesthetic techniques, such as using ultrasound guidance to place a needle near a nerve or fascial plane where nerves lie, and injecting local anesthetic helps numb those nerves that supply the breast tissue. One technique in particular that seemed promising for good breast analgesia perioperatively for these procedures is the PECS block. The PECS II block requires the injection of local anesthetic on the anterior chest wall between the pectoralis muscles and also between the pectoralis minor and serratus anterior muscles. The only problem is that nobody has really studied the effects of putting in a continuous catheter with those types of blocks. This would allow the block to be prolonged beyond the 12- to 24-hour postoperative period that is traditionally achieved by a traditional single-injection technique to up to three to five days.
I had the idea two or three years ago to combine two blocks and be able to place a catheter in one of the planes where we were injecting for the PECS block so we could extend the analgesia for days rather than just 24 hours. So I combined it with a block we would typically use for a brachial plexus block that’s used for upper extremity procedures. The new “combined” technique is called a Retroclavicular Approach to the PECS (RAP) block. The key is to insert the needle behind the clavicle, going underneath the clavicle and into the PECS plane instead of putting the needle directly on the anterior part of the chest or on the front of the chest wall. By doing that I’m able to place a catheter, have it come out behind the clavicle up near the trapezius muscle and it’s not in the surgical field anymore.
Another part of the research was to understand the spread of the injectate, or local anesthetic, which was conducted on cadavers. Since we don’t know what sensations the cadavers are feeling to assess injectate spread, we used a dye to inject into the PECS planes and had anatomists do dissections to tell us the spread we were able to achieve. The other thing we wanted to make sure of was that it was even possible to do this because there is a lot of pertinent vascular structures that are very close to the needle pathway to get to the plane. We performed the technique on four specimens and had a 100% success rate, including threading the catheters.
My passion and specialty in anesthesia is acute pain management. When I was studying at York College in the nurse anesthesia program, I had extensive rotations where I had the opportunity to do a lot of pain management, including regional anesthesia. So I finished the program with 450 to 500 blocks, which is a lot more than a typical student might have. As I continued to evolve my skill set and continued to want more knowledge, I saw that MTSA had launched the ASPM Fellowship. I applied, got accepted and now I’ve completed the program. As far as next steps go, I’m looking to fine-tune the research manuscript and submit it for publication.
President’s Message
Milestone Moments at MTSA

Chris Hulin
DNP, MBA, CRNA
President
One of the most rewarding aspects of leading an institution such as MTSA—which is filled with so many brilliant, passionate professionals—is witnessing “milestone moments” as they happen.
Just a few weeks ago, it occurred again. Some of our best and brightest achieved an honor that adds even more distinction in our effort to enhance the body of knowledge in nurse anesthesia and to produce evidence-based scholarship: Original research produced out of our Acute Surgical Pain Management Fellowship’s inaugural cohort was presented at the annual European Society of Regional Anaesthesia (ESRA) Congress, which took place in Dublin, Ireland.
As you can read in this edition of Airways, their research was chosen among countless other submissions and helped uncover new ways to improve patient care and outcomes, especially as it relates to surgical pain management and reducing the need for opioids. I couldn’t be more proud of these talented practitioners, and I’m confident that this marks the beginning of even more scholarship in this area.
With these research presentations at ESRA, our institution continues to demonstrate its commitment to supporting not only our own students and Fellows, but the wider CRNA community by creating evidence and scholarship related to acute surgical pain management. These efforts are also connected with the objective of reducing opioid consumption in operating rooms, which will help combat the harmful effects of these drugs in our communities.
We have been leading the charge for CRNA advancement in the surgical pain arena by:
- Becoming the first CRNA Center of Excellence in partnership with Halyard Health, training in acute pain management;
- Acquiring Neuraxiom.com in an effort to position MTSA as the lead resource in CRNA education and advancement in the acute surgical pain management arena;
- Joining with the AANA to develop the nation’s first and only clinically-based Acute Surgical Pain Management (ASPM) Fellowship;
- Offering dual enrollment for CRNAs in the Doctor of Nurse Anesthesia Practice (DNAP) and ASPM Fellowship programs, combining didactic and clinical learning;
- Advancing public policy work at the local, state and national level to advocate for the nurse anesthesia profession; and
- Developing a Surgical Pain Management Institute “think tank” to support the practicing CRNA with the creation of research and scholarship.
MTSA has always fostered a rich learning environment for our student body, and we continue to explore avenues for engagement with the working CRNA community. If you want to be more involved in these efforts—helping to identify partnerships, collaborators or funding sources—I encourage you to contact me at chris.hulin@mtsa.edu.
Mission Initiative Update
Teams provide expertise in Guyana and Haiti

MTSA President Chris Hulin (second from left) and students Elizabeth Gilbert and Warkim Giles (front row) conducted classroom review and simulations for nursing students in Guyana during the School’s recent Mission Initiative.

MTSA student Warkim Giles provides simulation instruction to nursing students at Georgetown Public Hospital System in Guyana.
MTSA’s mission team recently returned from Guyana, South America, after conducting test preparation and simulations for nursing students at Georgetown Public Hospital System.
“The trip was another great success. The Guyanese students continue to display eagerness to learn and enjoy the interaction with our students,” said President Chris Hulin.
MTSA students Elizabeth Gilbert and Warkim Giles led many of the simulations, while Hulin conducted review sessions for the students’ upcoming major exam before they enter into primary clinical education. According to Hulin, all the students were successful on the exam and are now busy learning in the OR.
“The trip was wonderful,” Gilbert said. “Warkim and I mainly went through different scenarios and OR simulations with the students. It was really rewarding seeing their thought processes and critical thinking progress through the week. Knowing that they are going to be the leaders in their country for future nurse anesthetists is a lot of pressure, but they are up for the challenge and will succeed.”
Giles added: “The Guyana mission trip was an awesome experience. It gave us the chance to impart the knowledge and skills we’ve learned at MTSA to the students in the CRNA program in Guyana. When you’re able to teach someone, I feel that you know the material. That was a nice confidence boost nearing the end of our program. I am extremely grateful for the opportunity to do God’s work in a foreign country. The skills they learned, or brushed up on, will greatly help them serve the people of Guyana.”
Haiti mission team provides acute surgical pain management
Six students, along with MTSA faculty and partners, are continuing the work of providing Acute Surgical Pain Management care alongside hand surgeons from the Touching Hands Project, at Hopital Adventiste d’Haiti in Carrefour, just outside the capital city of Port-au-Prince. As in past years, the team also is conducting education sessions for local doctors and nurses, helping to raise the standard of care and leave a long-term impact on the local population. The trip is planned for Oct. 7-13, 2018.
Funding for both the Guyana and Haiti mission trips was provided, in part, by the generous contributions of alumni and friends through the Mission and Awards Gala and other events and donations throughout the year. To contribute to MTSA’s Mission Initiatives, visit www.mtsa.edu/donate.
Sporting Clay Tournament
JOIN THE FUN AT THE 2ND ANNUAL
![]()
Friday, Nov. 9
7:30 a.m. – Registration
9:00 a.m. – Tournament Starts (all equipment provided)
Awards luncheon to follow (lunch included): Team awards for 1st, 2nd and 3rd place
Nashville Gun Club
Sporting Clay Complex
1100 County Hospital Rd.
Nashville, TN 37218
(Located off Briley Parkway, Bordeaux area)
Last year’s inaugural Sporting Clay Tournament provided an opportunity for marksmen and novices alike to aim for greatness at multiple shooting stations at the Nashville Gun Club. Lunch will be provided, and prizes are awarded for those who hit the most clays.
To register, visit www.mtsa.edu/sportingclay.
Proceeds from this event support MTSA’s Mission Initiatives in Haiti, Guyana and local communities.
Basic Cadaveric Ultrasound-Guided Regional Anesthesia Workshop
Limited slots available for CRNAs
Nov. 2 – Registration Closes
Nov. 4 – Course Date
 The eight-hour Basic Cadaveric Ultrasound-Guided Regional Anesthesia Workshop is a hands-on, basic training course utilizing cadavers and “live” scanning models, state-of-the-art ultrasound technology, and a comprehensive, highly-practical approach to regional anesthesia techniques for surgery and acute pain management.
The eight-hour Basic Cadaveric Ultrasound-Guided Regional Anesthesia Workshop is a hands-on, basic training course utilizing cadavers and “live” scanning models, state-of-the-art ultrasound technology, and a comprehensive, highly-practical approach to regional anesthesia techniques for surgery and acute pain management.
Bill Johnson, DNAP, CRNA, Director, MTSA Acute Surgical Pain Management Fellowship, along with fellow instructors Stace Dollar, MS, CRNA, and John Edwards, MS, CRNA, will teach interscalene, supraclavicular, infraclavicular, axillary, distal upper and lower extremity salvage, fascia iliaca, femoral, adductor canal, and popliteal blocks using the “Maverick Method.”
Participants will receive the benefits of small-group needling stations, low faculty-to-attendee ratios, and an individualized learning plan that suits the attendees’ needs in regional anesthesia.
More information and registration is available at www.mtsa.edu/basiccadaveric.
2019 workshop dates announced
MTSA has released its schedule for the 2019 Cadaveric Ultrasound-Guided Regional Anesthesia Workshops. Dates are listed below, and more information is available at www.mtsa.edu/non-degree.
Feb. 17
April 7
Aug. 4
Class of 2018 Graduation Ceremony
MTSA graduation exercises for the Class of 2018 are scheduled for Friday, Nov. 16, 2018, at the Madison Campus Seventh-day Adventist Church. The ceremony recognizing this year’s graduates will begin at 10 a.m.
Ken Wetmore, Senior Pastor, Madison Campus Seventh-day Adventist Church, will offer the homily.
The event will be followed by an open house on the School’s campus located adjacent to the church. Refreshments will be served.
MTSA alumni ballot mailed
The ballot to elect 2019 MTSA Alumni Officers and Decade Representatives has been mailed to all MTSA alumni. In accordance with MTSA Alumni Association Bylaws, this ballot must be returned and in-hand at the MTSA Alumni Office by close-of-business on Nov. 7 to be counted. The ballot includes the following nominees:
President: Rod Schwindt (2001)
Secretary: Trevor Eldred (2003) and Brad Irby (2003)
Representative for 2010-Present: Mya Davidson (2017) and Samantha Porter (2011)
Representative for 1990s: Richard R. Lane (1992)
Representative for 1980s: Danny Denning (1985) and Tommy Tucker (1988)
Representative-At-Large: Wade Rippy (2000) and Michael York (2007)
All MTSA Alumni are invited to attend the MTSA Alumni Association Business meeting to confirm the ballot results. This meeting will be held at MTSA on Tuesday, Nov. 13, at 4:30 p.m. (CST) in the Magan Building. If you have any questions, please call (615) 732-7674 or e-mail jclosser@mtsa.edu.
MTSA grad wins title at North America Beauty Pageant

MTSA graduate Joannie Summers, MS, was crowned 2018 Elite North America titleholder. (Photo credit: Matty Jacobson of Magic Dreams Productions)
Courtesy of Spring Hill Advertiser News
MTSA 2004 graduate Joannie Summers, MS, was crowned 2018 Elite North America® titleholder at a pageant held in June in Orlando, representing Tennessee.
Joannie resides in Spring Hill, Tenn., with her husband Carey Amorine, a retired veteran who served 20 years in the U.S. Army working as a medic in Special Forces. Together they have six children ages 29, 27, 26, 23, 13 and 11. She has a 3-year-old grandchild and one on the way.
She graduated from Spalding University with a Bachelor of Science degree in Nursing and from MTSA with a Master of Science degree in Nursing Anesthesia. Currently she is working with an anesthesia group at a hospital in Columbia, and she also works in two office surgery centers as the sole anesthesia provider in Dickson and Franklin, Tenn.
Her volunteer work includes 13 years with the Mid-Cumberland Head Start program including two years on the policy council. This past year she was elected to serve on the Board of Directors for the Mid-Cumberland Community Action Agency, which is a nonprofit organization providing resources that promote self-sufficiency for low income families in Middle Tennessee.
Class of 2020 recognized at White Coat Ceremony


The ceremony celebrating DNAP students’ progression to clinical rotations was held on Thursday, Aug. 16, at the Madison Campus Seventh-day Adventist Church and streamed on Facebook Live
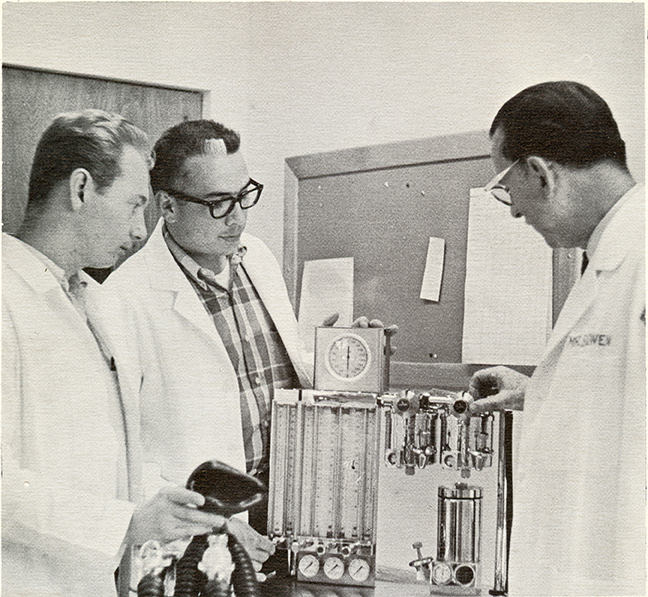
From the Archives
Flow Meter Functions Explained
This photo of MTSA’s founder appeared in The Nashville Tennessean newspaper on June 11, 1967. The caption read: “Bernard V. Bowen, CRNA, DSc (right), chief anesthetist and head of the training program at Madison Hospital, explaining the functions of flow meters to students John W. Moore Jr. (left) and Richard Frezza.”